Aftercare
Following surgery, the patient is instructed in the care of the stoma, placement of the ileostomy bag, and necessary changes to diet and lifestyle. Because the large intestine (a site of fluid absorption) is no longer a part of the patient's digestive system, fecal matter exiting the stoma has a high water content. The patient must therefore be diligent about his or her fluid intake to minimize the risk of dehydration. Visits with an enterostomal therapist (ET) or a support group for individuals with ostomies may be recommended to help the patient adjust to living with a stoma. Once the ileostomy has healed, a normal diet can usually be resumed, and the patient can return to normal activities.
Risks
Risks associated with the ileostomy procedure include excessive bleeding, infection, and complications due to general anesthesia. After surgery, some patients experience stomal obstruction (blockage), inflammation of the ileum, stomal prolapse (protrusion of the ileum through the stoma), or irritation of the skin around the stoma.
Normal results
The physical quality of life of most patients is not affected by an ileostomy, and with proper care most patients can avoid major medical complications. Patients with a permanent ileostomy, however, may suffer emotional aftereffects and benefit from psychotherapy.
Morbidity and mortality rates
Among patients who have undergone a Brooke ileostomy, medical literature reports a 19–70% risk of complications. Small bowel obstruction occurs in 15% of patients; 30% have problems with the stoma; 20–25% require further surgery to repair the stoma; and 30% experience postsurgical infections. The rate of complications is also high among patients who have had a continent ileostomy (15–60%). The most common complications associated with this procedure are small bowel obstruction (7%), wound complications (35%), and failure to restore continence (50%). The mortality rate of both procedures is less than 1%.
Alternatives
Patients with mild to moderate ulcerative colitis may be able to manage their disease with medications. Medications that are given to treat ulcerative colitis include enemas containing hydrocortisone or mesalamine; oral sulfasalazine or olsalazine; oral corticosteroids; or cyclosporine and other drugs that affect the immune system.
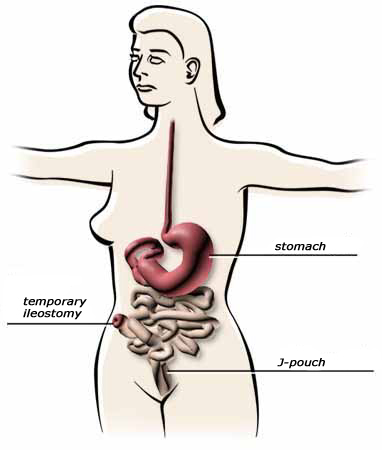
A surgical alternative to ileostomy is the ileal pouch-anal anastomosis, or ileoanal anastomosis. This procedure, used more frequently than permanent ileostomy in the treatment of ulcerative colitis, is similar to a continent ileostomy in that an ileal pouch is formed. The pouch, however, is not attached to a stoma but to the anal canal. This procedure allows the patient to retain fecal continence. An ileoanal anastomosis usually requires the placement of a temporary ileostomy for two to three months to give the connected tissues time to heal.
BOOKS
"Inflammatory Bowel Diseases: Ulcerative Colitis." In The Merck Manual of Diagnosis and Therapy, edited by Mark H. Beers, MD, and Robert Berkow, MD. Whitehouse Station, NJ: Merck Research Laboratories, 1999.
Pemberton, John H., and Sidney F. Phillips. "Ileostomy and Its Alternatives" (Chapter 105). In Sleisenger and Fordtran's Gastrointestinal and Liver Disease, 7th ed. Philadelphia: Elsevier Science, 2002.
Rolandelli, Rolando H., and Joel J. Roslyn. "Colon and Rectum," (Chapter 46), In Sabiston Textbook of Surgery. Philadelphia: W. B. Saunders Company, 2001.
PERIODICALS
Allison, Stephen, and Marvin L. Corman. "Intestinal Stomas in Crohn's Disease." Surgical Clinics of North America 81, no. 1 (February 1, 2001): 185-95.
ORGANIZATIONS
Crohn's and Colitis Foundation of America. 386 Park Ave. S., 17th Floor, New York, NY 10016. (800) 932-2423. .
United Ostomy Association, Inc. 19772 MacArthur Blvd., Suite 200, Irvine, CA 92612-2405. (800) 826-0826. .
OTHER
Hurst, Roger D. "Surgical Treatment of Ulcerative Colitis." [cited May 1, 2003]. .
Stephanie Dionne Sherk
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Ileostomies are usually performed in a hospital operating room. The surgery may be performed by a general surgeon, a colorectal surgeon (a medical doctor who focuses on diseases of the colon, rectum, and anus), or gastrointestinal surgeon (a medical doctor who focuses on diseases of the gastrointestinal system).
QUESTIONS TO ASK THE DOCTOR
- Why is an ileostomy being recommended?
- What type of ileostomy would work best for me?
- What are the risks and complications associated with the recommended procedure?
- Are any nonsurgical treatment alternatives available?
- How soon after surgery may I resume my normal diet and activities?
Page:
<> 1 2