
New or changing symptoms often mean that additional treatment is needed to keep ulcerative colitis under control. For this reason, people who have ulcerative colitis should be in frequent contact with their physicians. Common symptoms that require a doctor's immediate attention are fever, which could indicate infection or a ruptured intestine, and heavy bleeding from the rectum. A serious, but uncommon, complication, called megacolon, results when the colon inflammation is so severe that it stops the colon's motion. Megacolon causes the abdomen to swell, which can cause vomiting or severe abdominal pain and bloating. Megacolon requires emergency treatment.
Showing posts with label About Ulcerative Colitis. Show all posts
Showing posts with label About Ulcerative Colitis. Show all posts
Friday, April 17, 2009
Thursday, April 9, 2009
How Serious Is Ulcerative Colitis
People who live with ulcerative colitis are burdened by many questions, especially when they are having their first crisis and being diagnosed. These questions focus on issues of pain, symptoms, possible complications and disability
The answers to many questions are not apparent and often take a long time to determine. But most people who live with ulcerative colitis have increasingly longer periods when they feel well than they do when they are acutely ill. And this has never been more true than today, when doctors have an increasingly large arsenal of treatment options.
Moreover, the severity of the illness varies greatly for different people. One long-term study suggests that after the first attack, less than 10 percent develop chronic, longstanding, persistent symptoms, while the rest go into complete remission, and remain symptom free.
The most common concerns of people diagnosed with ulcerative colitis deal with the issues of:
Determining The Severity Of The Disease
The severity of the disease can be measured objectively by determining symptoms such as:
- The number of stools in a day
- Appetite
- Fever
- The number of days in a month when an individual must modify his or her work, home, or social schedule because of diarrhea, fatigue, fever, and other symptoms
It can also be measured subjectively, through questioning by a doctor of an individual's general state of being, such as whether that person is angry, depressed, in pain, embarrassed by needing to use the toilet frequently in social or business situations.
The severity of the objective signs seen on x-rays does not necessarily correspond to how severe the subjective symptoms are. One individual with disease that looks severe on radiological exam might have the ability to lead a relatively normal life, while another person with few objective signs of disease may find the conditions totally debilitating, both physically and mentally.
Can Ulcerative Colitis Cause Serious Complications?
In some people, ulcerative colitis can cause serious complications that include:
- Severe bleeding that may require blood transfusions
- Toxic megacolon, a dangerous condition where the colon becomes extremely distended (swollen), causing a person to become severely ill, with a distended belly and a high fever. The colon expands and becomes paralyzed. Occasionally, it may rupture. If this occurs, up to 30 percent may not survive it. The diagnosis is confirmed by simple x-ray of the abdomen.
- Perforation (a hole in the colon), which can cause widespread infection and can be life threatening
Not everyone who has ulcerative colitis will experience complications from the illness, however. In cases where a first attack comes on very suddenly, complications will occur in about 10 percent of individuals. Effective treatments are available for these complications.
Need To Know: Q. Is ulcerative colitis life threatening? A. Ulcerative colitis is very rarely life threatening. Cases of toxic megacolon or excessive bleeding due a very severe The |
Possible Increased Risk Of Colon Cancer
Individuals with ulcerative colitis have a slightly increased risk of developing colorectal cancer. The increase in risk is dependent on the amount of colon involved. The incidence is greatest for those with ![]()
The risk of colon cancer developing, according to various studies, is estimated at 5 percent to 10 percent after 10 years, rising to 15 percent to 40 percent after 30 years
Thus, for individuals with ulcerative colitis, the risk of developing colorectal cancer increases over time, as is true for the general population. Therefore, regular screenings--either a ![]()
![]()
| Nice To Know: Scientists are still searching for the link between ulcerative colitis and colon cancer.
|
|
Ulcerative Colitis
Classifying Ulcerative Colitis
In individuals with ulcerative colitis, a distinct portion of the colon is diseased. Disease starts at the rectum and moves "up" the colon to involve more of the organ. Doctors categorize ulcerative colitis by the amount of colon involved. Regardless of how little or how much of the colon is involved, symptoms can vary from mild to severe in any individual.
Types of ulcerative colitis are:
-
Ulcerative proctitis : If ulcerative colitis is limited to the rectum, it is known as ulcerative proctitis. Symptoms are diarrhea, bloody stool, pain in the rectal area, and a sense of urgency to empty the bowel.
Proctosigmoiditis : If ulcerative colitis affects the rectum and the sigmoid colon, it is known as proctosigmoiditis. Symptoms are diarrhea, bloody stool, cramps and pain in the rectal area, and moderate pain on the left side of the abdomen.
Left-sided colitis : Left-sided colitis affects the entire left side of the colon, from the rectum to the place where the colon bends near the spleen and begins to run across the upper abdomen (the splenic flexure). Symptoms include diarrhea, bleeding, weight loss and loss of appetite, and sometimes severe pain on the left side of the abdomen.
Pancolitis : If the entire colon is affected, the term pancolitis is used ("pan" meaning total). The classification is most important in planning treatment. While ulcerative proctitis, proctosigmoiditis, and even left-sided colitis can be treated with local agents introduced through the anus, including steroid-based or other enemas and foams, pancolitis must be treated with oral medication so that active ingredients can reach all of the affected portions of the colon.
Wednesday, April 8, 2009
Frequently Asked Questions
Here are some frequently asked questions related to ulcerative colitis.
Q: Is ulcerative colitis an autoimmune disease?
A: There is certainly a malfunction in the immune system that takes place in ulcerative colitis. However, immunosuppressive medications used to keep individuals from rejecting transplanted organs have shown less effectiveness in treating ulcerative colitis than in treating Crohn's disease.
Q: Is ulcerative colitis life threatening?
A: Ulcerative colitis is very rarely life threatening. Cases of toxic megacolon or excessive bleeding due a very severe ![]()
![]()
Q: If both parents have ulcerative colitis, what are the chances that their children will have ulcerative colitis?
A: Ulcerative colitis is not a strictly genetic disease. To date, scientists have found no specific gene that miscodes and causes ulcerative colitis. The chances of a child having ulcerative colitis if his or her parents do is only slightly greater than the chances of any child having ulcerative colitis.
Q: If I need surgery, will I have to wear an ![]()
A: Not necessarily. There are three options for eliminating bowel waste after removal of the colon. One is the standard ostomy, and use of ostomy appliances. Another is a so-called continent ostomy, which is emptied through a rigid tube you insert through the valve-like ostomy opening. The third is the ileo-anal pull-through, where the ileum is attached to the rectal wall, and you eliminate through the anus.
Q: Should I be worried about steroid treatment?
A: ![]()
Q: Are diagnostic tests to find out if I have ulcerative colitis painful?
A: A ![]()
![]()
![]()
Q: Should I be worried about colon cancer if I have ulcerative colitis?
A: Statistical evidence does show that people with ulcerative colitis do have a slightly higher incidence of colon cancer than the general population. For this reason, doctors begin regularly screening those with colitis eight years after diagnosis. Those with ![]()
Q: My 11-year-old was just diagnosed with ulcerative colitis. I thought only adults could get the disease. Does my child face any special obstacles in having the disease treated?
A: In the last quarter century, it has become clear that ulcerative colitis affects large numbers of children and young teens. Nutritional deficiency is a major issue in treatment of children with ulcerative colitis. Children are growing machines, and although ![]()
Sunday, April 5, 2009
Ulcerative Colitis
When To Call A Professional
New or changing symptoms often mean that additional treatment is needed to keep ulcerative colitis under control. For this reason, people who have ulcerative colitis should be in frequent contact with their physicians. Common symptoms that require a doctor's immediate attention are fever, which could indicate infection or a ruptured intestine, and heavy bleeding from the rectum. A serious, but uncommon, complication, called megacolon, results when the colon inflammation is so severe that it stops the colon's motion. Megacolon causes the abdomen to swell, which can cause vomiting or severe abdominal pain and bloating. Megacolon requires emergency treatment.
Wednesday, March 4, 2009
Travel Tips
When you have ulcerative colitis (UC), traveling can be stressful. But with a little planning, you can have a stress-free trip.
- Find a doctor in the town or towns you will be visiting. Your regular doctor can help you locate someone in the cities you will be visiting.
- Make sure you have enough medication. Call your doctor and ask for a refill of your prescription.
- Talk to your doctor about a plan of action in case you experience a flare-up while away.
When you're en route, whether it's by car or plane, these tips can help make your traveling relaxing.
- Always carry your medication with you. If you are traveling by plane, pack your medication in your carry-on bag.
- If you are flying or traveling by bus or train, request an aisle seat for easy access.
- Talk to some friends who have been to the city or attraction, and try to find the best bathrooms.
Wednesday, February 18, 2009
Ulcerative Colitis Glossary
Abscess: A pocket or collection of pus.
Anemia: Lower than normal amounts of hemoglobin in the red cells of the blood.
Arthritis: Inflammation of a joint, accompanied by pain, swelling, heat, or redness.
Autoimmunity: An inflammatory reaction to one's own tissues.
Barium Enema: An x-ray examination of the colon and rectum after liquid barium has been infused through the rectum.
Biopsy: A small piece of tissue taken from the body for examination under the microscope.
Colectomy: Removal of part or all of the colon.
Colon: The large intestine.
Colonoscopy: A test in which a flexible, lighted tube is inserted through the rectum to examine the colon.
Colostomy: A surgically created opening of the colon to the abdominal wall, allowing the diversion of fecal waste.
Continent Ileostomy: The surgical creation of a pouch inside the lower abdomen to collect waste. No external appliance is required; the pouch is emptied regularly with a small tube inserted through a nipple opening in the abdomen.
Distension: An uncomfortable swelling feeling in the abdomen, often caused by excessive amounts of gas and fluids in the intestine.
Endoscopy : The examination of the inside of a hollow organ, such as the bowel, using special lighted tubes.
Erythema Nodosum : Red swellings occasionally seen on the lower legs during flareups of Crohn's disease and ulcerative colitis.
Exacerbation: An aggravation of symptoms or an increase in disease activity; a relapse.
Excision: Surgical removal.
Fissure: A crack in the skin, usually in an area of the anus in Crohn's disease.
Fistula: An abnormal channel occuring between two loops of intestine, or between the intestine and another structure, such as the bladder, vagina, or skin.
Folic Acid: One of the vitamins responsible for the maintenance of red blood cells.
Gastroenterologist: A physician specially trained in the diagnosis and treatment of patients with gastrointestinal disease.
Gut: General word for intestine or bowel.
Hemorrhage: Abnormally heavy bleeding.
IBD: Acronym for inflammatory bowel disease.
Idiopathic: Of unknown cause.
Ileostomy: A surgically created opening of the abdominal wall to the ileum, allowing the diversion of fecal waste.
Ileum: The lower third of the small intestine, adjoining the colon.
Inflammatory Bowel Disease (IBD): A collective term for Crohn's disease and ulcerative colitis.
Irritable Bowel Syndrome : Altered motility of the small and large intestine, causing diarrhea and abdominal discomfort. Sometimes mistakenly called "spastic colitis," this condition does not cause inflammation of the colon and has no relationship to ulcerative colitis.
Lactose Deficiency/Lactose Intolerance: A condition caused by a decrease or absence of the enzyme lactase, which aids in the digestion of milk sugar (lactose).
Leukocytosis: An increased number of white blood cells in circulation
Motility: Movement of the muscles that propel food through the intestinal tract.
Mucus: A whitish substance produced by the intestine, which may be found in the stool.
Obstruction: A blockage of the small or large intestine that prevents the normal passage of intestinal contents.
Ostomy: The surgical creation of an artifical excretory opening, such as a colostomy.
Perforation: Formation of a hole in the bowel wall, allowing intestinal contents to enter the abdominal cavity.
Peristalsis: Normal rhythmic movements of the stomach and intestine.
Peritonitis: Inflammation of the peritoneum (the membrane enclosing the abdominal organs), usually resulting from an intestinal perforation.
Proctectomy : Removal of the rectum.
Proctitis: Inflammation of the rectum.
Proctocolectomy: Removal of the entire colon and rectum.
Regional Enteritis: Another name for Crohn's disease affecting the small intestine.
Remission: A lessening of symptoms and a return to good health.
Resection: Surgical removal of a diseased portion of intestine.
Short Bowel Syndrome: A condition in which so much diseased bowel has been surgically removed that the remaining intestine can no longer absorb sufficient nutrients.
Sigmoidoscopy: A test in which a lighted tube is passed through the rectum into the sigmoid colon.
Small Bowel: Small intestine.
Stenosis: A narrowing of an area (e.g., a segment of intestine).
Stoma: A surgically created opening of the bowel onto the skin, the result of ostomy surgery.
Stricture : A narrowed area of intestine caused by active inflammation or scar tissue.
Tenesmus: A persistent urge to empty the bowel, usually caused by inflammation of the rectum.
Toxic Megacolon: Acute dilation of the colon in colitis (or occasionally in Crohn's disease), which may lead to perforation.
Upper G.I. Series: An x-ray exam of the esophagus, stomach, and duodenum performed in the fasting patients after the ingestion of liquid barium. The duration of the exam can be prolonged to allow for visualization of the entire small intestine, including the terminal ileum. The x-ray is then known as an upper G.I. series with small-bowel follow-through.
Anemia: Lower than normal amounts of hemoglobin in the red cells of the blood.
Arthritis: Inflammation of a joint, accompanied by pain, swelling, heat, or redness.
Autoimmunity: An inflammatory reaction to one's own tissues.
Barium Enema: An x-ray examination of the colon and rectum after liquid barium has been infused through the rectum.
Biopsy: A small piece of tissue taken from the body for examination under the microscope.
Colectomy: Removal of part or all of the colon.
Colon: The large intestine.
Colonoscopy: A test in which a flexible, lighted tube is inserted through the rectum to examine the colon.
Colostomy: A surgically created opening of the colon to the abdominal wall, allowing the diversion of fecal waste.
Continent Ileostomy: The surgical creation of a pouch inside the lower abdomen to collect waste. No external appliance is required; the pouch is emptied regularly with a small tube inserted through a nipple opening in the abdomen.
Distension: An uncomfortable swelling feeling in the abdomen, often caused by excessive amounts of gas and fluids in the intestine.
Endoscopy : The examination of the inside of a hollow organ, such as the bowel, using special lighted tubes.
Erythema Nodosum : Red swellings occasionally seen on the lower legs during flareups of Crohn's disease and ulcerative colitis.
Exacerbation: An aggravation of symptoms or an increase in disease activity; a relapse.
Excision: Surgical removal.
Fissure: A crack in the skin, usually in an area of the anus in Crohn's disease.
Fistula: An abnormal channel occuring between two loops of intestine, or between the intestine and another structure, such as the bladder, vagina, or skin.
Folic Acid: One of the vitamins responsible for the maintenance of red blood cells.
Gastroenterologist: A physician specially trained in the diagnosis and treatment of patients with gastrointestinal disease.
Gut: General word for intestine or bowel.
Hemorrhage: Abnormally heavy bleeding.
IBD: Acronym for inflammatory bowel disease.
Idiopathic: Of unknown cause.
Ileostomy: A surgically created opening of the abdominal wall to the ileum, allowing the diversion of fecal waste.
Ileum: The lower third of the small intestine, adjoining the colon.
Inflammatory Bowel Disease (IBD): A collective term for Crohn's disease and ulcerative colitis.
Irritable Bowel Syndrome : Altered motility of the small and large intestine, causing diarrhea and abdominal discomfort. Sometimes mistakenly called "spastic colitis," this condition does not cause inflammation of the colon and has no relationship to ulcerative colitis.
Lactose Deficiency/Lactose Intolerance: A condition caused by a decrease or absence of the enzyme lactase, which aids in the digestion of milk sugar (lactose).
Leukocytosis: An increased number of white blood cells in circulation
Motility: Movement of the muscles that propel food through the intestinal tract.
Mucus: A whitish substance produced by the intestine, which may be found in the stool.
Obstruction: A blockage of the small or large intestine that prevents the normal passage of intestinal contents.
Ostomy: The surgical creation of an artifical excretory opening, such as a colostomy.
Perforation: Formation of a hole in the bowel wall, allowing intestinal contents to enter the abdominal cavity.
Peristalsis: Normal rhythmic movements of the stomach and intestine.
Peritonitis: Inflammation of the peritoneum (the membrane enclosing the abdominal organs), usually resulting from an intestinal perforation.
Proctectomy : Removal of the rectum.
Proctitis: Inflammation of the rectum.
Proctocolectomy: Removal of the entire colon and rectum.
Regional Enteritis: Another name for Crohn's disease affecting the small intestine.
Remission: A lessening of symptoms and a return to good health.
Resection: Surgical removal of a diseased portion of intestine.
Short Bowel Syndrome: A condition in which so much diseased bowel has been surgically removed that the remaining intestine can no longer absorb sufficient nutrients.
Sigmoidoscopy: A test in which a lighted tube is passed through the rectum into the sigmoid colon.
Small Bowel: Small intestine.
Stenosis: A narrowing of an area (e.g., a segment of intestine).
Stoma: A surgically created opening of the bowel onto the skin, the result of ostomy surgery.
Stricture : A narrowed area of intestine caused by active inflammation or scar tissue.
Tenesmus: A persistent urge to empty the bowel, usually caused by inflammation of the rectum.
Toxic Megacolon: Acute dilation of the colon in colitis (or occasionally in Crohn's disease), which may lead to perforation.
Upper G.I. Series: An x-ray exam of the esophagus, stomach, and duodenum performed in the fasting patients after the ingestion of liquid barium. The duration of the exam can be prolonged to allow for visualization of the entire small intestine, including the terminal ileum. The x-ray is then known as an upper G.I. series with small-bowel follow-through.

Monday, July 14, 2008
Potential Problems After Surgery
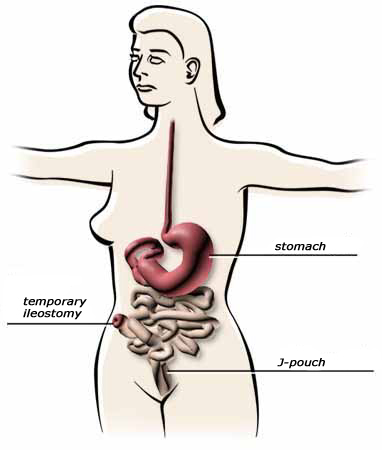
Many people are concerned about the longevity of their jpouch. How long will it last? What types of complications might potentially occur? Here is a link to an excellent site that gives you really good in-depth and objective info on the Potential Problems Following J-Pouch Surgery
Image to the left shows the large intestine and rectum removed, the formation of the temporary ileostomy, and the jpouch. The whole series of photos can be found by clicking on the following jpouch.org link.
Interactive Tutorial on UC
This is a great Interactive Ulcerative Colitis Tutorial. It is pretty basic info, but it is comprehensive and it is really easy to follow. Plus, there is a cool explanation how food goes through the digestive system.
Info from Medline Plus.
Sunday, July 6, 2008
Meet: "True Guts" - The Movie

Crohn’s & UC Disease FILM
Crohn's Disease
A very inspirational movie to those living with Crohn’s Disease or Colitis and has received attention from various medical authorizes nationwide (e.g. Crohn's and Colitis Foundation of America).
http://www.trueguts.com
View Trailer...
About Movie...
A very inspirational movie to those living with Crohn’s Disease or Colitis and has received attention from various medical authorizes nationwide (e.g. Crohn's and Colitis Foundation of America).
http://www.trueguts.com
View Trailer...
About Movie...
For the first time ever, Crohn's Disease and colitis are being thrust into public awareness through a nationwide inspirational movie, True Guts: Struggle and Triumph over Crohn's Disease and Ulcerative Colitis.
True Guts is the story of what happens when individuals turn life altering Crohn's Disease and Colitis into a personal springboard to get more out of life. True Guts depicts individuals (including teenagers and young adults) with Crohn's or colitis and how each of them found ways to use his/her disease to improve their lives. Also included is advice from a nationally recognized gastroenterologist and psychiatrist, each breaking down the steps that are necessary to take control of your life with chronic diseases such as Crohn's or Colitis.
Watch film trailer here.
Watch film trailer here.
Monday, March 10, 2008
Crohn's Disease - Surgery
Surgery is rarely done for Crohn's disease and it is not a cure. When surgery is needed, as little of the intestines as possible is removed to preserve normal function. The disease tends to return in areas that were previously not affected, and you may need surgery again.
Surgery may be needed for Crohn's disease if no medicine can control your symptoms, you have serious side effects from medicines, your symptoms can be controlled only with long-term use of corticosteroids, or you develop complications such as fistulas, abscesses, or bowel obstructions.
Surgery may be needed when you have:
- Bowel blockage (obstruction).
- Abscesses or tears (fissures) in the anal area or when abnormal connections (fistulas) form between two parts of the intestine or between the intestine and other internal organs.
- Holes (perforations) in the large intestine.
- Cancer or precancerous tissue.
- Severe disease that does not respond to other treatment.
- Severe bleeding that requires ongoing blood transfusions.
Surgery Choices
Surgery is not usually done for Crohn's disease. If you do have surgery, it will most likely be one of the following:
- Resection: The diseased portion of the intestines is removed, and the healthy ends of the intestine are reattached. Resection surgery does not cure Crohn's disease, which often comes back near the site of surgery.
- Proctocolectomy and ileostomy: The surgeon removes the large intestine and rectum
 , leaving the lower end of the small intestine (the ileum). The anus is sewn closed, and a small opening called a stoma is made in the skin of the lower abdomen. The ileum is connected to the stoma, creating an opening to the outside of the body, where stool empties into a small plastic pouch called an ostomy bag that is applied to the skin around the stoma.
, leaving the lower end of the small intestine (the ileum). The anus is sewn closed, and a small opening called a stoma is made in the skin of the lower abdomen. The ileum is connected to the stoma, creating an opening to the outside of the body, where stool empties into a small plastic pouch called an ostomy bag that is applied to the skin around the stoma. - Strictureplasty: The surgeon makes a lengthwise cut in the intestine and then sews the opening together in the opposite direction. This makes the intestine wider and helps with obstruction of the bowels. This is sometimes done at the same time as resection, or when a person has had resection in the past. Strictureplasty is used when the doctor is trying to save as much of the intestines as possible.
Another procedure that may be done is balloon dilation. This is not a surgery. The doctor runs an endoscope through your intestines from your anus. The endoscope is a long, thin tube that has a video camera on the end. Next, the doctor uses the endoscope to thread an uninflated balloon across the stricture (the narrowed part of the intestine). When the balloon is inflated, it makes that part of the intestine wider. The balloon is deflated and then removed. Balloon dilation is a new technique and not as much is known about its long-term success compared to the surgical procedures listed above. Balloon dilation might be done if you want to put off a more complicated surgery for a while or if you have had surgery before and the doctor wants to save as much of the intestines as possible.
What To Think About
These surgeries can be done on children. Surgery can improve a child's well-being and quality of life and restore normal growth and sexual development.
In rare cases, intestinal transplant is used to treat Crohn's disease. In this complex procedure, the small intestine is removed and replaced with the small intestine of a person who has recently died and donated his or her organs.
In very rare cases, when the risk of other surgery is high, bypass surgery may be done to preserve the bowel. In this procedure, the intestine is cut above the diseased area and reconnected to a healthy section below the diseased area. The diseased part of the intestine remains but is no longer used. This surgery is not done often because the diseased loop remains and may cause problems later.
WebMD Medical Reference from Healthwise
Via: http://www.webmd.com
Surgery
Ulcerative colitis affects only the large intestine, so surgery that removes the entire large intestine can cure the disease. Some people who have ulcerative colitis in the entire colon (pancolitis) eventually need surgery to remove the colon.
People may need surgery for ulcerative colitis in several situations, such as when other therapy fails to manage symptoms, when holes develop in the large intestine, or if dysplasia is found during colonoscopy or biopsy.

Surgery Choices
Removal of the colon to cure ulcerative colitis involves one of these surgeries:
- In ileoanal anastomosis, the surgeon removes some or all of the large intestine (colon) and the diseased lining of the rectum. Then the end of the small intestine (the ileum) is connected to the anal canal. The anal sphincters are saved and this allows you to have bowel movements without an ostomy.
- In proctocolectomy and ileostomy, the large intestine and rectum are removed, leaving the lower end of the small intestine (the ileum). The surgeon sews the anus closed and makes a small opening called a stoma in the skin of the lower abdomen. The ileum is connected to the stoma, creating an opening to the outside of the body. Stool empties into a small plastic pouch called an ostomy bag that is applied to the skin around the stoma.
- In continent ileostomy, the surgeon removes the large intestine (colon) and creates a pouch and a valve from the lower end of the small intestine (the ileum). The surgeon then connects the valve to an opening (stoma) in the skin of the lower abdomen. After this surgery, you can insert a tube into the valve to release stool from the intestines.
What To Think About
Ileoanal anastomosis is performed most often. Proctocolectomy with ileostomy is preferred for people who cannot tolerate anesthesia for a long period of time because of illness or age.
Both children and adults may have ileoanal anastomosis, which may be done in stages to reduce the risk of complications. A temporary ileostomy is created first, with the ileum pouch completed 3 to 6 months later. Surgery can improve a child's well-being and quality of life and restore normal growth and sexual development.
In the past, many people who had surgery for IBD had an ileostomy and wore an ostomy bag outside the abdomen. Newer surgeries like ileoanal anastomosis or continent ileostomy can eliminate the need for an ostomy bag with fairly good results when they are done by a trained surgeon. Traditional ostomy surgery is easier and may have fewer risks and complications than the newer procedures, but some people may be less satisfied with the results.
People with ulcerative colitis may choose to have their colon removed because their symptoms cause a poor quality of life. They also may want the surgery to prevent the possibility of colon cancer.
In most cases, surgery can be scheduled at your convenience. Emergency surgery usually is not needed unless an acute attack causes toxic megacolon, severe uncontrolled bleeding, or a spontaneous rupture in the intestine. The risk of complications after surgery can be high if surgery is done during a severe or rapidly worsening attack or if emergency surgery is needed. If toxic megacolon has developed, surgery may be the only option to save a person's life.
WebMD Medical Reference from Healthwise
Via: http://www.webmd.com
Ulcerative Colitis Guide
- Overview & Facts
Ulcerative colitis is one of the most common forms of inflammatory bowel disease. Learn what it is -- and what you can do to control it.
What is Ulcerative Colitis?
Get an overview of ulcerative colitis, one of the most common inflammatory bowel diseases.
Ulcerative colitis causes inflammation and sores in the lining of the large intestine.
Causes
It's not clear just what causes ulcerative colitis.
Are You at Risk?
Genetic factors can increase your risk of ulcerative colitis.
Prevention
While you can't prevent ulcerative colitis, you can take steps to reduce its severity.
- Symptoms & Types
Symptoms
Symptoms of ulcerative colitis can include diarrhea, constipation, and pain.
Warning Signs
Call your doctor right away if you experience any of these symptoms.
The diagnosis of ulcerative colitis is suggested by the symptoms, yet other diagnostic tests help determine and confirm this disease. Read more.
Diagnosis
Here are the exams and tests doctors use to diagnose and evaluate ulcerative colitis.
- Treatment & Care
Treatment
Treatment for ulcerative colitis depends on the severity of the disease. It usually includes medications to control symptoms, along with changes in diet.
If your symptoms are mild, anti-diarrheal medications and changes in diet may help.
Medications are usually the treatment of choice for ulcerative colitis.
In some situations, people may need surgery for ulcerative colitis.
Most alternative or complementary treatments for ulcerative colitis have not been proven to work.
Here are factors to consider when deciding whether to have surgery for ulcerative colitis.
- Living & Managing
Ulcerative colitis can be controlled, but it's important to follow your doctor's advice.
Living & Coping
Follow these tips for proper care for your ostomy
To learn more about ulcerative colitis -- and to find support groups -- these resources can help.
Finding Help
Here's where to find more information about ulcerative colitis.
Resources
References for articles on ulcerative colitis used in this guide.
Credits for articles on ulcerative colitis used in this guide.
This information can help you take an active role in managing and treating ulcerative colitis.
- Glossary
Glossary Terms for Inflammatory Bowel Disease
If you can't quite understand all the terms your doctor uses to describe IBD (ulcerative colitis and Crohn’s disease) print out this glossary and take it to your next appointment. Together you can explore what you need to know to help achieve the best treatment possible.
Inflammatory Bowel Disease Glossary
- Frequently Asked Questions
- What is inflammatory bowel disease (IBD)?
-
Answer:
Inflammatory bowel disease is a group of two diseases: ulcerative colitis and Crohn's disease. These chronic illnesses can inflame the gastrointestinal tract, causing bloody diarrhea, abdominal pain, and weight loss. Ulcerative colitis can affect the entire large intestine or the rectum. Crohn's disease mainly affects short segments of both the small and large intestine.
- What is Crohn’s disease?
-
Answer:
Crohn’s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn’s disease can affect any area of the GI tract, from the mouth to the anus, but it most commonly affects the lower part of the small intestine, called the ileum. The swelling extends deep into the lining of the affected organ. The swelling can cause pain and can make the intestines empty frequently, resulting in diarrhea.
- Who gets Crohn’s disease?
-
Answer:
Crohn’s disease affects men and women equally and seems to run in some families. About 20% of people with Crohn’s disease have a blood relative with some form of inflammatory bowel disease, most often a brother or sister and sometimes a parent or child. Crohn’s disease can occur in people of all age groups, but it is more often diagnosed in people between the ages of 20 and 30. People of Jewish heritage have an increased risk of developing Crohn’s disease, and blacks are at decreased risk for developing Crohn’s disease.
- What causes inflammatory bowel disease?
-
Answer:
The cause(s) of inflammatory bowel disease is not known. However people believe that it may be genetically linked since IBD is known to run in families.
An environmental cause is also believed to play a role in developing Crohn's disease because it is most often occurs in people who smoke, are residents of Northern European countries and live in urban areas.
Other researchers speculate that the disease may be caused by an infection or virus.
Still others believe that the body's immune system is reacting to unidentified or unknown antigens. This antigen would cause the immune system to respond inappropriately against normal intestinal tissue, resulting in chronic inflammation. - What diseases/infections or vaccines are thought to be linked to the development of IBD?
-
Answer:
Measles, mumps, or rubella virus infection is not known to cause IBD. The virus that causes measles infects the respiratory system and then spreads to lymphatic tissue (an important part of the immune system). During the acute infection, lymph cells in the gastrointestinal tract are infected, but whether this causes chronic inflammation is highly questionable.
One theory speculates that measles virus may persist in the intestine in certain individuals and later trigger a chronic inflammatory infection; however, this has not been proven. Because the measles, mumps, and rubella (MMR) vaccine contains a very weak live measles virus it has been suggested that the vaccine could cause an inflammatory process in the intestine. This theory has not been proven and is speculative.
- What are the symptoms?
-
Answer:
The most common symptoms of Crohn’s disease are abdominal pain, often in the lower right area, and diarrhea. Rectal bleeding, weight loss, arthritis, skin problems, and fever may also occur. Bleeding may be serious and persistent, leading to anemia. Children with Crohn’s disease may suffer delayed development and stunted growth. The range and severity of symptoms varies.
- How are Crohn's disease and ulcerative colitis diagnosed?
-
Answer:
A thorough physical exam and a series of tests may be required to diagnose Crohn’s disease or ulcerative colitis.
The doctor may do an upper GI series to look at the small intestine. For this test, the person drinks barium, a chalky solution that coats the lining of the small intestine, before X-rays are taken.The doctor may also do a visual exam of the colon by performing either a sigmoidoscopy or a colonoscopy. For both of these tests, the doctor inserts a long, flexible, lighted tube linked to a computer and TV monitor into the anus.
The doctor may also do a biopsy, which involves taking a sample of tissue from the lining of the intestine to view with a microscope.
- What are the complications of Crohn's disease?
-
Answer:
The most common complication is blockage of the intestine. Blockage occurs because the disease tends to thicken the intestinal wall with swelling and scar tissue, narrowing the passage.
Crohn’s disease may also cause sores, or ulcers, that tunnel through the affected area into surrounding tissues, such as the bladder, vagina, or skin.
Nutritional complications are common in Crohn’s disease. These deficiencies may be caused by inadequate dietary intake, intestinal loss of protein, or poor absorption, also referred to as malabsorption.
Other complications associated with Crohn’s disease include arthritis, skin problems, inflammation in the eyes or mouth, kidney stones, gallstones, or other diseases of the liver and biliary system. Some of these problems resolve during treatment for disease in the digestive system, but some must be treated separately.
- What is ulcerative colitis?
-
Answer:
Ulcerative colitis is a disease that causes inflammation and sores, called ulcers, in the lining of the rectum and colon. Ulcers form where inflammation has killed the cells that usually line the colon, then bleed and produce pus. Inflammation in the colon also causes the colon to empty frequently, causing diarrhea.
- Who gets ulcerative colitis?
-
Answer:
Ulcerative colitis can occur in people of any age, but it usually starts between the ages of 15 and 30, and less frequently between 50 and 70 years of age. It affects men and women equally and appears to run in families, with reports of up to 20% of people with ulcerative colitis having a family member or relative with ulcerative colitis or Crohn’s disease. A higher incidence of ulcerative colitis is seen in whites and people of Jewish descent.
- What are the symptoms of ulcerative colitis?
-
Answer:
The most common symptoms of ulcerative colitis are abdominal pain and bloody diarrhea. Patients also may experience
- anemia
- fatigue
- weight loss
- loss of appetite
- rectal bleeding
- loss of body fluids and nutrients
- skin lesions
- joint pain
- growth failure (specifically in children)
About half of the people diagnosed with ulcerative colitis have mild symptoms. Others suffer frequent fevers, bloody diarrhea, nausea, and severe abdominal cramps.
- What are the other complications associated with ulcerative colitis?
-
Answer:
Ulcerative colitis may also cause problems such as arthritis, inflammation of the eye, liver disease, and osteoporosis. It is not known why these problems occur outside the colon. Scientists think these complications may be the result of inflammation triggered by the immune system. Some of these problems go away when the colitis is treated.
- What causes ulcerative colitis?
-
Answer:
Many theories exist about what causes ulcerative colitis. People with ulcerative colitis have abnormalities of the immune system, but doctors do not know whether these abnormalities are a cause or a result of the disease. The body’s immune system is believed to react abnormally to the bacteria in the digestive tract.
Ulcerative colitis is not caused by emotional distress or sensitivity to certain foods or food products, but these factors may trigger symptoms in some people. The stress of living with ulcerative colitis may also contribute to a worsening of symptoms. -
Answer:
Treatment may include drugs, nutrition supplements, surgery, or a combination of these options. Treatment for Crohn’s disease depends on the location and severity of disease, complications, and the person’s response to previous medical treatments when treated for reoccurring symptoms. Many of the treatments are used for both conditions.
Someone with inflammatory bowel disease may need medical care for a long time, with regular doctor visits to monitor the condition.
- What drug therapies are available?
-
Answer:
Anti-Inflammation Drugs. Most people are first treated with drugs containing mesalamine, a substance that helps control inflammation. Sulfasalazine is the most commonly used of these drugs. Patients who do not benefit from it or who cannot tolerate it may be put on other mesalamine-containing drugs, generally known as 5-ASA agents, such as Asacol, Dipentum, or Pentasa. Possible side effects of mesalamine-containing drugs include nausea, vomiting, heartburn, diarrhea, and headache.
Cortisone or Steroids. Cortisone drugs and steroids—called corticosteriods—provide very effective results. Prednisone is a common generic name of one of the drugs in this group of medications. In the beginning, when the disease it at its worst, prednisone is usually prescribed in a large dose. The dosage is then lowered once symptoms have been controlled. These drugs can cause serious side effects, including greater susceptibility to infection.
Immune System Suppressors. Drugs that suppress the immune system are also used to treat Crohn’s disease. Most commonly prescribed are 6-mercaptopurine or a related drug, azathioprine. Immunosuppressive agents work by blocking the immune reaction that contributes to inflammation. These drugs may cause side effects like nausea, vomiting, and diarrhea and may lower a person’s resistance to infection.
Infliximab (Remicade). This drug is the first of a group of medications that blocks the body’s inflammation response. The FDA approved the drug for the treatment of moderate to severe Crohn’s disease that does not respond to standard therapies (mesalamine substances, corticosteroids, immunosuppressive agents) and for the treatment of open, draining fistulas. Infliximab, the first treatment approved specifically for Crohn’s disease, is a TNF substance.
Antibiotics. In inflammatory bowel disease antibiotics are used to treat bacterial overgrowth in the small intestine caused by stricture, fistulas, or prior surgery. For this common problem, the doctor may prescribe one or more of the following antibiotics: ampicillin, sulfonamide, cephalosporin, tetracycline, or metronidazole.
Anti-Diarrheal and Fluid Replacements. Diarrhea and crampy abdominal pain are often relieved when the inflammation subsides, but additional medication may also be necessary. Several antidiarrheal agents could be used, including diphenoxylate, loperamide, and codeine. Patients who are dehydrated because of diarrhea will be treated with fluids and electrolytes.
- What type of nutrition supplementation is needed?
-
Answer:
The doctor may recommend nutritional supplements, especially for children whose growth has been slowed. Special high-calorie liquid formulas are sometimes used for this purpose.
- Is surgery ever required to treat or cure this condition? And why do some people with the condition require surgery while others do not?
-
Answer:
Two-thirds to three-quarters of patients with Crohn’s disease will require surgery at some point in their lives. About 25% to 40% of ulcerative colitis patients must eventually have their colons removed because of massive bleeding, severe illness, rupture of the colon, or risk of cancer.
Surgery becomes necessary when medications can no longer control symptoms. Surgery is used either to relieve symptoms that do not respond to medical therapy or to correct complications such as blockage, perforation, abscess, or bleeding in the intestine. Surgery to remove part of the intestine can help people with Crohn’s disease, but it is not a cure. Surgery does not eliminate the disease as inflammation tends to return to the area next to where the diseased intestine was removed.
In ulcerative colitis, surgery maybe needed to remove the colon and/or rectum.
- Is colon cancer a concern with ulcerative colitis?
-
Answer:
About 5% of people with ulcerative colitis develop colon cancer. The risk of cancer increases with the duration of the disease and how much the colon has been damaged. For example, if only the lower colon and rectum are involved, the risk of cancer is no higher than normal. However, if the entire colon is involved, the risk of cancer may be as much as 32 times the normal rate.
Sometimes precancerous changes occur in the cells lining the colon. These changes are called "dysplasia." People who have dysplasia are more likely to develop cancer than those who do not. Doctors look for signs of dysplasia when doing a colonoscopy or sigmoidoscopy and when examining tissue removed during these tests.According to the 2002 updated guidelines for colon cancer screening, people who have had IBD throughout their colon for at least eight years and those who have had IBD in only the left colon for 12 to 15 years should have a colonoscopy with biopsies every 1 to 2 years to check for dysplasia. Such screening has not been proven to reduce the risk of colon cancer, but it may help identify cancer early. These guidelines were produced by an independent expert panel and endorsed by numerous organizations, including the American Cancer Society, the American College of Gastroenterology, the American Society of Colon and Rectal Surgeons, and the Crohn’s & Colitis Foundation of America.
WebMD Health News
Subscribe to:
Posts (Atom)










